Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124
Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124
Rewrite the content and keep the original meaning and format, and add 5 more H2, the content is “
The development of the apex locators has evolved from its first generation to now the 6th generation of the apex locator. From resistance type in 1st generation, impedance type in 2nd generation the frequency type in 3rd generation, nowadays the latest generation of electronic apex locators (Sixt generation) are using multi-frequency to be more precise and accurate.
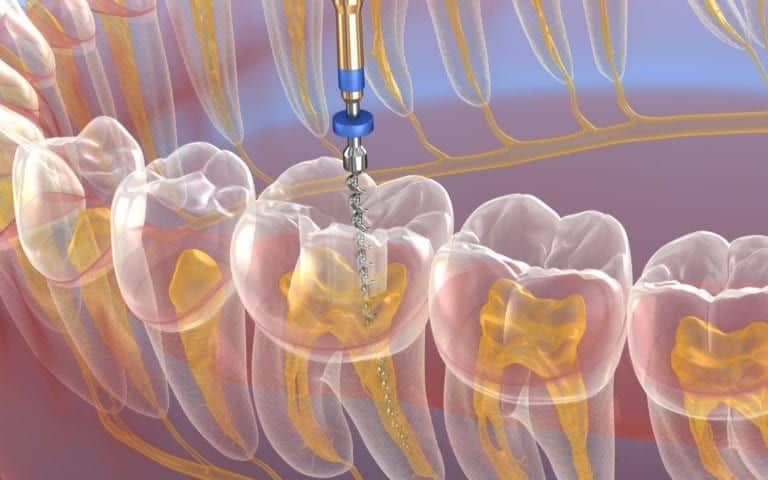
Electronic apex locators (EALs) use the human body to produce an electrical circuit. They have two sides: one is connected to the endodontic file in the root canal, and the other is connected to the patient’s lip. The electrical circuit will be complete when the tip of the dental file reaches the periodontal tissue. These devices are particularly useful for patients with gag reflex problems or those who cannot tolerate radiography films or sensors. Because each generation of apex locators has a distinct display, they show different images of the apical region.
Endo measurement is one of the key factors responsible for the success of endodontic therapy. Electronic determination of working length has gained enormous popularity, owing to its extreme accuracy and predictability. The literature is flooded with the self-proclaimed generations of the apex locators. However, the categorization in chronological order has somehow always been confusing. One of the convenient methods of segregating the apex locators is based on dividing them into different generations.
This guide is aimed at a concise description of the actual scientific rationale behind the so-called “generations”, to help dentists better understand the latest developments in apex locators techniques.
The adoption of electronic apex locators (EALs) for determining working length has gained popularity, and these locators are categorized into different generations.
Currently, first and second generation apex locators are not in production anymore.
Advancements in dental science and technology led to the development of subsequent generations, including the third, fourth, fifth, and a modified version of the fifth generation known as the sixth generation, exhibiting enhanced accuracy in working length measurement.
This particular classification is entirely based on the working principles of the apex locators. The clinical correlation can be interpreted from the fact that the more the machine can work in extreme environments and the more accurate it is, the better it is for dental professionals.
These apex locators use the resistance method for determining the WL. Basically, these instruments measured the opposition to the flow of direct current (resistance) hence the name Resistance apex locators. Initially, first-generation EALs, known as resistance apex locators, utilized direct current (resistance) to measure the apical area, causing discomfort to patients due to high currents. However, they were found to be less accurate compared to radiography methods, representing a significant drawback.
In response, second-generation EALs, referred to as impedance-based apex locators, were introduced with modifications to improve accuracy. These devices utilized alternating current (impedance) for apex detection, addressing some of the limitations of the first generation, yet they still lacked a digital read-out and faced accuracy challenges in the presence of electroconductive irrigations and tissue fluids. Second generation units utilize the current of a single frequency to perform the task.
Third-generation apex locators employed a dual frequency, utilizing the “ratio method” to measure canal length accurately during endodontic therapy. The ratio method involved simultaneous measurements of impedance values at two frequencies (high – 8 kHz and low – 400 Hz), calculating a quotient that indicated the file’s location in the canal. However, the dual frequency method had the drawback of requiring calibration for each canal before use.
In contrast, the fourth generation could not process impedance values mathematically. This generation of apex locators uses multiple frequencies (2-5 frequencies) to measure the impedance to determine the WL[9]. The multi-frequency measurement system is used to calculate the distance from the tip of the file to the foramen by measuring changes in impedance between two electrodes separately measured capacitance and resistance. The next step is comparing them with a database to identify the narrowest part of the root. The fourth generation is generally considered to perform well in relatively dry canals.
Fifth-generation EALs brought about advantages such as safety, reliability, clinician and patient friendliness, and accurate detection of working length, especially in the presence of exudates or weeping in the canal. However, even if 5th generation performs very well in the presence of blood and exudate they experience considerable difficulties while operating in dry canals
The sixth generation, also termed adaptive apex locators, represents a modification of the fifth generation and exhibits the highest consistency in measurements, particularly in cases of root perforation or apical root resorption. Measurement with the adaptive apex locator has made it possible to eliminate the necessity of drying or moistening the canal. The precision of readings in this generation is not affected by the presence of blood, sodium hypochlorite, or while manipulating dry canals. One of the specific characteristics of this generation is that those units can continuously adapt to the level of humidity in the root canal.
”